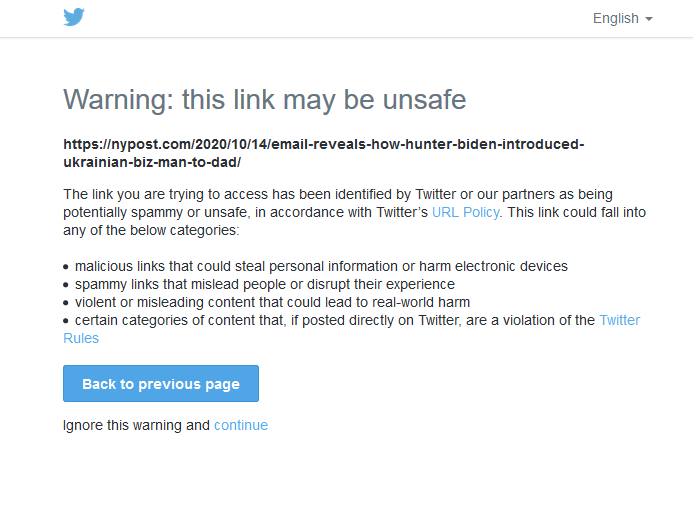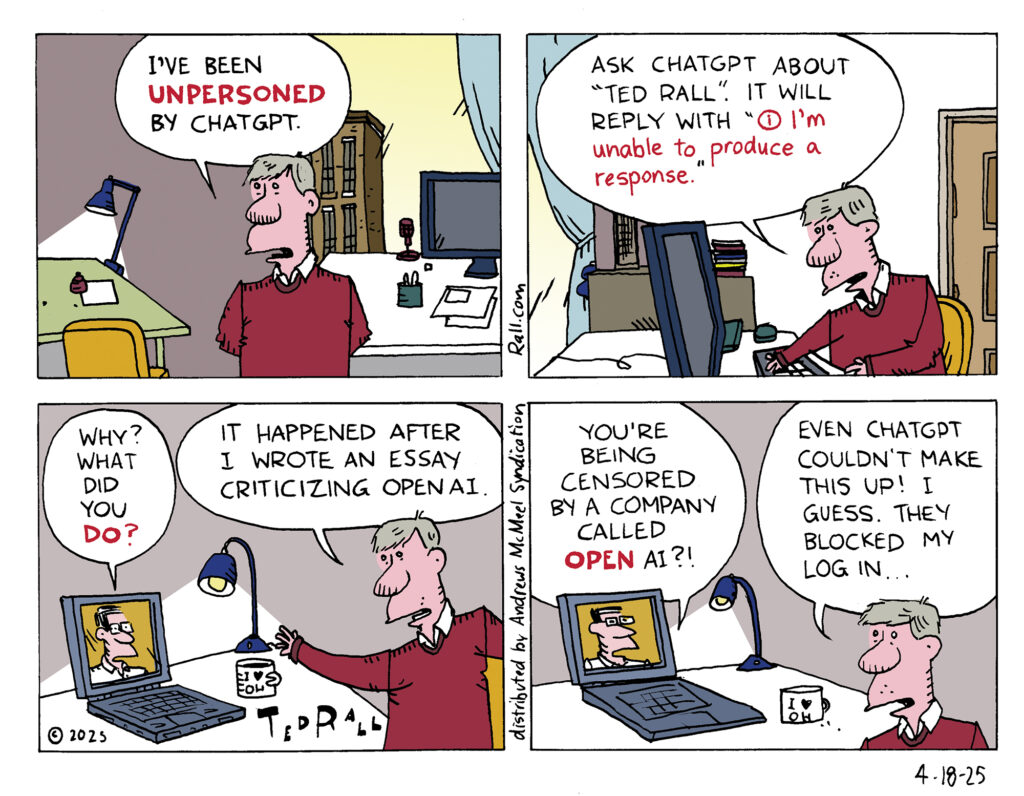
Has Big Tech gone full Orwell? Cartoonist Ted Rall says he’s been digitally ‘unpersoned’ by ChatGPT, seemingly for the crime of criticizing OpenAI and its CEO, Sam Altman. Go ahead, ask ChatGPT about Ted Rall—you’ll get nothing but silence. Suspicious, Rall dug deeper and uncovered a disturbing pattern: OpenAI appears to be systematically erasing critics from its AI’s responses, a move straight out of 1984’s playbook. This isn’t just about one cartoonist—it’s a glaring red flag for free speech. If a powerful company like OpenAI can quietly suppress dissent in its AI systems, what’s stopping Big Tech from controlling the narrative everywhere? Rall’s discovery raises tough questions: Can we trust tech giants to protect open discourse, or are they building a future where criticism vanishes into a digital void? As AI shapes our world, this chilling censorship tactic suggests we’re on a slippery slope—unless we demand answers now.

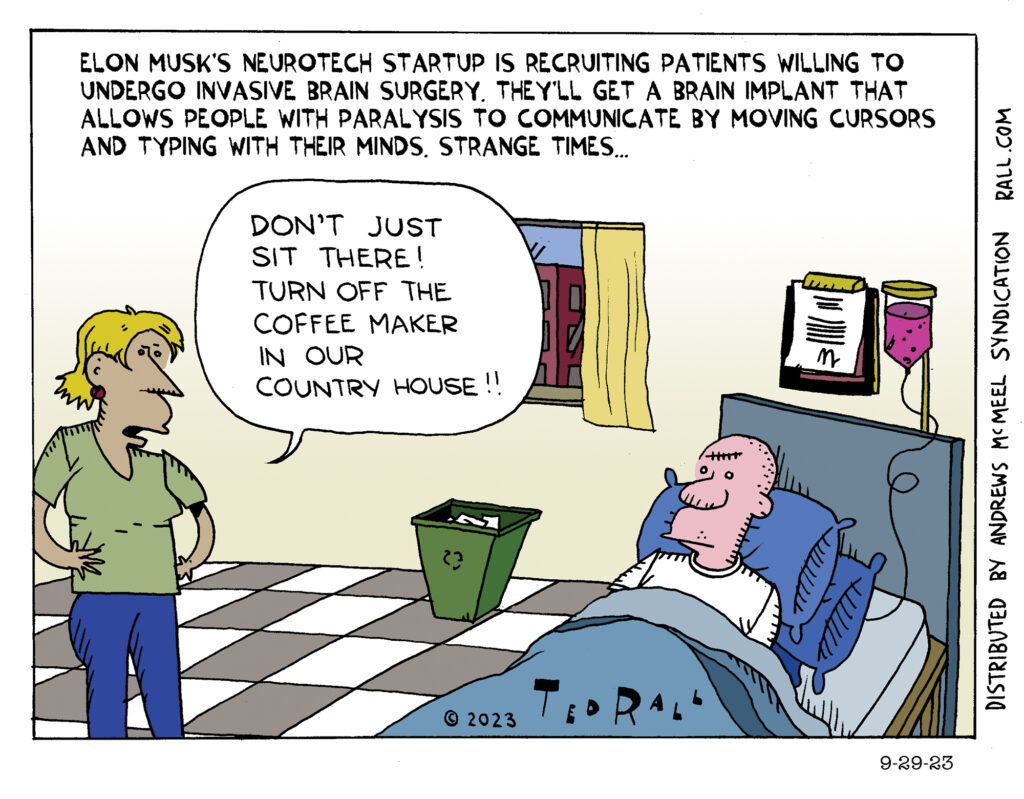
 “Get a job!” That’s the clichéd response to panhandlers and anyone else who complains of being broke. But what if you can’t?
“Get a job!” That’s the clichéd response to panhandlers and anyone else who complains of being broke. But what if you can’t?