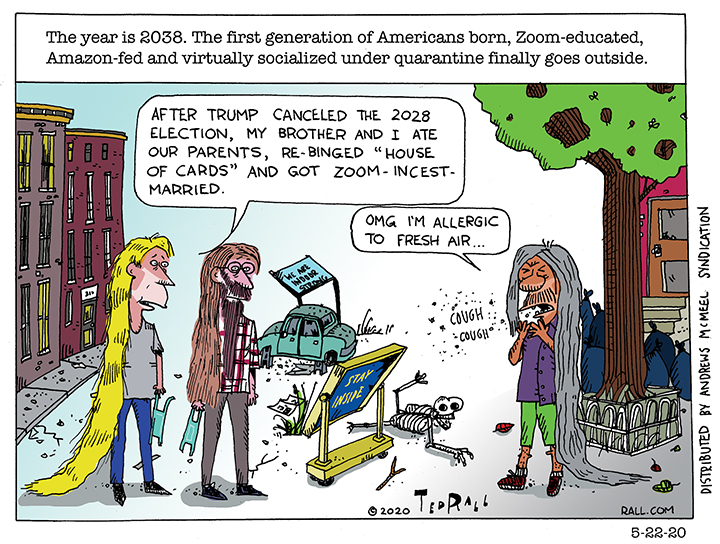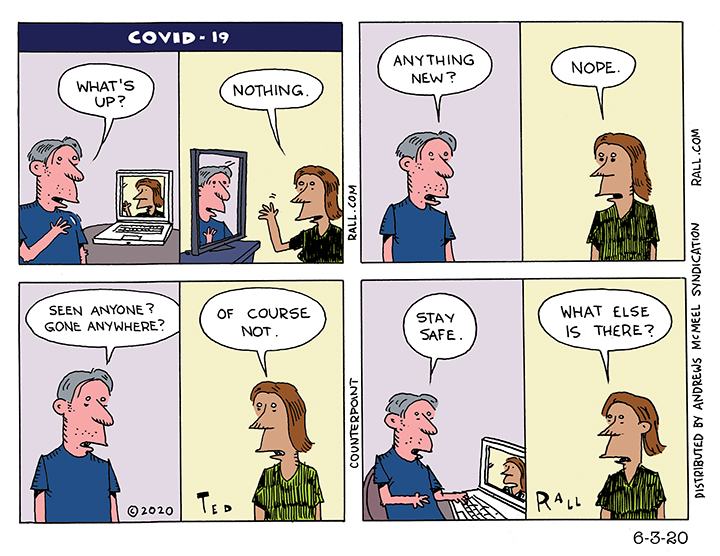
The word “quarantine” comes from the Italian term for 40 days because that was the longest time that people were believed to be able to withstand lockdown before they started to lose it. Now we are starting to see why. Is it really life if you can’t live it?