
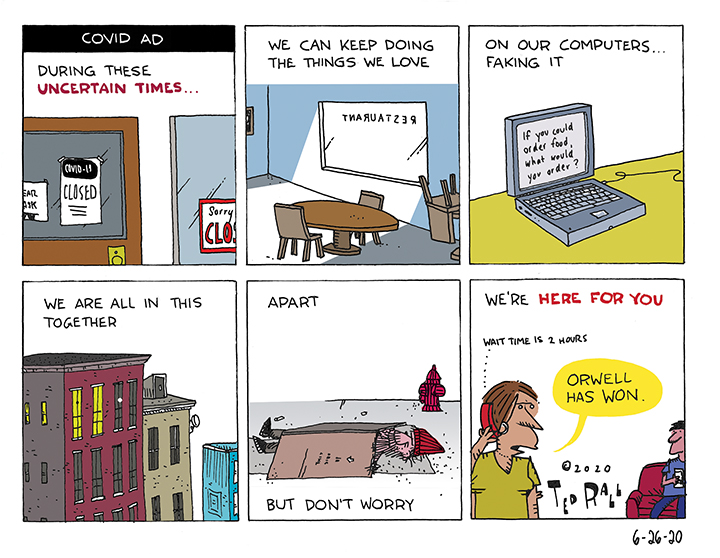
You know how the ads go. They have THAT music. Some somber narrator comes on and announces that during these “uncertain times” given “what’s going on” that some corporation that never cared about you actually does.
You know how the ads go. They have THAT music. Some somber narrator comes on and announces that during these “uncertain times” given “what’s going on” that some corporation that never cared about you actually does.

COVID-19 has created the ideal medium for a summer of continuous protest.
Political protest demonstrations used to be weekend affairs in which angry leftists shouted at empty government offices before shuffling home Sunday afternoon to gear up for the workweek. With one out of four workers having filed for unemployment and many more working from home, tens of millions of Americans have free time to march in the streets. Sporting events, movie theaters, retail stores and even houses of worship are closed due to the coronavirus lockdown.
The usual distractions of a leap year are absent; the summer Olympics are canceled and presidential campaigning is so close to nonexistent as to be irrelevant. Politics is no longer about the politicians. Politics is in the street, where there’s nothing to do but gather, chant and dodge teargas cannisters.
The vacuum created by the lockdown and the impotence of a political class that no longer pretends to lead during a staggering medico-economic crisis has been filled by Black Lives Matter following the murder of George Floyd. BLM has won important symbolic victories like the toppling of Confederate statues and a renewed push to remove the Stars and Bars from the Mississippi state flag. As the movement against police brutality and institutional racism continues, look for more substantive systemic reforms in policing.
What comes next? The eviction and foreclosure resistance movement.
Thanks to Congress’ reluctance to pass another big stimulus package, protests in general will continue into the foreseeable future. But they won’t all be against evil cops. A looming eviction and foreclosure crisis could broaden the struggle from one centered around racial grievances into a class-based fight for economic justice.
Courts are about to get flooded by eviction hearings. 30% of Americans missed their June housing payment. Supplemental $600-per-week unemployment checks expire July 31st.
“I think we will enter into a severe renter crisis and very quickly,” Columbia Law professor Emily Benfer, a housing expert who tracks eviction policies, told The New York Times May 30th. Without government action, she warned, “we will have an avalanche of evictions across the country.”
There is no sign that the government will lift a finger to help people who lost their jobs and will soon face homelessness. Even Elizabeth Warren and Bernie Sanders, the most progressive members of the U.S. Senate, refuse to consider a rent or mortgage payment holiday. They support a tepid “moratorium,” not a rent freeze. Under a moratorium back rent would pile up and all come due at once later on. Millions of people would be kicked outside this winter during a possible “second wave” of COVID-19. That’s the best scenario. Odds are, there won’t even be a moratorium. Congress will do little to nothing to help struggling tenants and homeowners.
Millions of homeowners and renters displaced from their homes during the 2008-09 subprime mortgage meltdown received zero assistance from the government. There were no protests worth mentioning. This time will be different.
First, there’s safety in numbers. The scale of this eviction crisis is much bigger. Three times more people have lost their jobs than during the Great Recession, during a much shorter period of time. Members of an eviction resistance movement can help one another block county sheriffs from kicking them out. Among those who are still working, the tenuous nature of the labor market has everyone in there-but-for-the-grace-of-God-go-I mode. We are in this together.
Second, this economic cataclysm wasn’t some act of God. People were ordered to shelter in place by the government. That’s why they lost their jobs, not a seemingly random stock market fluctuation. Targets of eviction and foreclosure won’t internalize any shame. They know they haven’t done anything wrong. They social distanced as asked; why should they sleep on the streets now because public health officials required them to go without income?
Third, Black Lives Matter has demonstrated the efficacy of street protests and of grassroots solidarity. Cops are currently about as popular as an STD. How enthusiastically will police respond to a landlord’s request to fight their way through an angry crowd to throw a family onto the street? It depends on the municipality. Things will quickly turn ugly.
Finally, memories of how the big banks squandered their Bush-Obama bailouts on exorbitant CEO salaries and renovating luxurious executive washrooms are still fresh. Even on the right, it will be tough to garner political support for banks trying to remove homeowners whose only crime was following stay-at-home orders.
There is a long but now largely forgotten history of tenant resistance movements in this country, mostly led by the communist Left. Each 1st of the month between now and this fall brings us closer to a new radical struggle between people who ask nothing more than to keep a roof over their heads and a system that prioritizes the right to own and control property over the most basic of human needs.
That movement will bring us closer to revolution.
(Ted Rall (Twitter: @tedrall), the political cartoonist, columnist and graphic novelist, is the author of “Political Suicide: The Fight for the Soul of the Democratic Party.” You can support Ted’s hard-hitting political cartoons and columns and see his work first by sponsoring his work on Patreon.
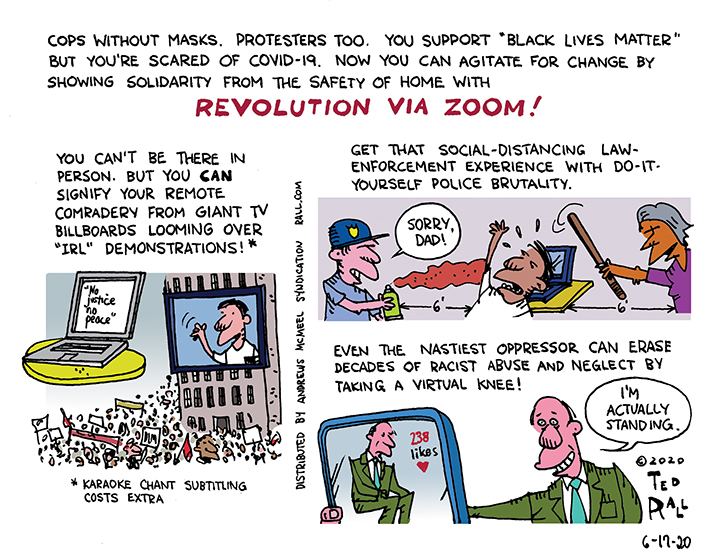
Cops without masks. Cops too. Agitate for Black Lives Matter from the safety of your home.
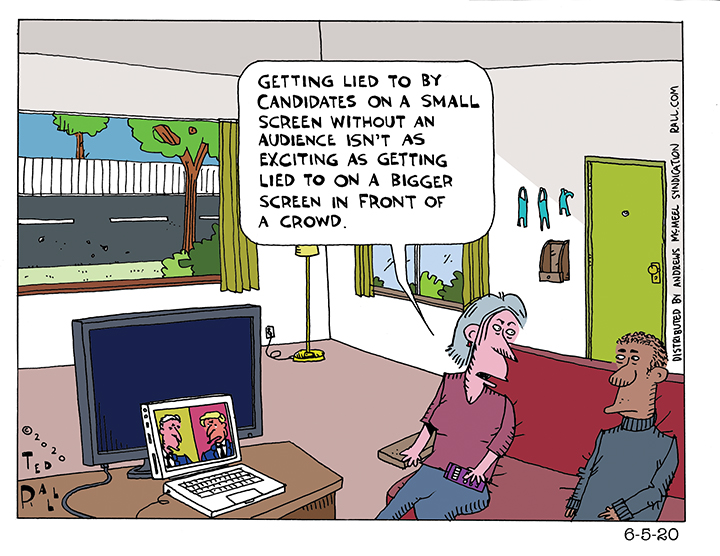
Can Joe Biden win a presidential campaign from his basement on a small screen without anyone watching? We’re about to find out. Of course, it’s not like most people ever get to interact with the candidates anyway. It’s just that television seems more “real” than the Internet.
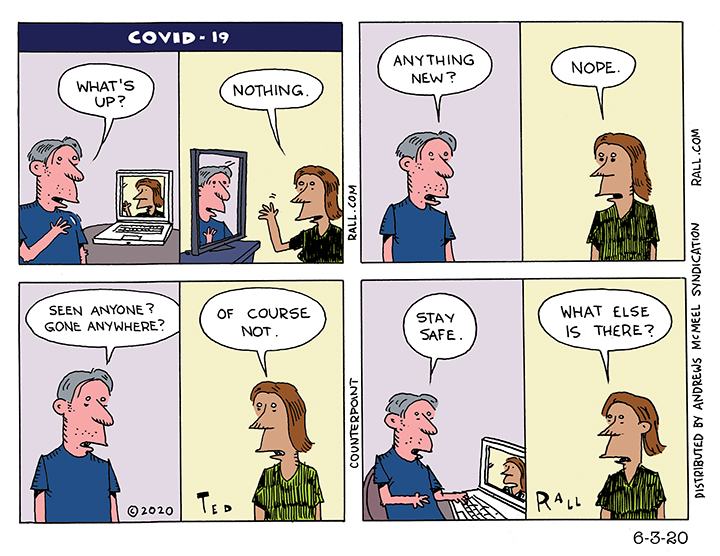
The word “quarantine” comes from the Italian term for 40 days because that was the longest time that people were believed to be able to withstand lockdown before they started to lose it. Now we are starting to see why. Is it really life if you can’t live it?
Few things are more terrifying than the unknown, as we are discovering as we struggle to navigate, avoid and (if we fail) survive a mysterious new virus. That goes double when reliable information is hard to come by; it is unquantifiably worse without credible leadership.
“Who ya gonna believe,” Chico Marx asked, “me or your own eyes?” More than other cultures of which I am aware, Americans are acculturated to ignore their instincts and the truth of their observations. A smoker might wake up coughing up phlegm every morning for decades yet he only begins to internalize that tobacco is dangerous to his health after a surgeon general he has never met issues a report. You might live in the same house years on end but discount your observation of the fact that it used to snow but now it doesn’t; global warming only becomes official when hundreds of climate scientists certify what you already knew.
Sometimes you have to trust yourself.
Even when you are mistaken about some details.
I’m 90% sure that I had COVID-19. It was in November. I was in LA for several weeks. In March I blogged about my symptoms: “I had an incessant dry cough…I had a constant fever. My temperature ranged from about 101° during the day to closer to 103° at night. My chest was tight: it felt like a car was parked on it. I had absolutely no energy whatsoever. I was exhausted. Even walking half a block, I had to take a break. I would get back to my hotel after a meeting and be asleep by 6 PM. I would sleep 14 hours and wake up still wiped out. ‘What the hell,’ I would ask myself, ‘is going on?’”
I tested negative for influenza. An x-ray revealed early-stage pneumonia. I was prescribed antibiotics and a nebulizer. Obviously I recovered; here I am writing this. But I’m still weak and tired.
If I could prove I had the novel coronavirus in November, it might be a news story. Aside from a New Jersey mayor who says he is sure that he had COVID-19 in November and a 55-year-old Chinese man whom doctors say had the disease on November 17th, the scientific and journalistic consensus is that the coronavirus pandemic originated in Wuhan, China in December. Last week my physician administered a serology test to determine if I have antibodies consistent with past infection with SARS-CoV-2. It came back negative. I was puzzled. If I hadn’t had COVID-19, or the flu, what the hell was this horrible illness?
I’m 56. I’ve had trouble with my lungs my entire life: asthma, lots of bronchitis, several cases of pneumonia, swine flu. My symptoms are remarkably consistent. My November experience was nothing like anything before. What bronchitis gives you fever for weeks at a time? What pneumonia?
The day after my doctor called with the negative antibody test result, the FDA issued a statement essentially declaring such lab tests worthless for the purpose of figuring out whether you’ve ever had COVID-19. So even if it had come back positive, it wouldn’t have meant anything.
Even if my test had been 100% reliable, and it had come back positive, all the test result would have proven is that I had COVID-19 at some point. It would not have evidenced that I contracted COVID-19 in November. I could have caught something else in November and COVID-19 asymptomatically, later.
Further reducing my reliability as a possible COVID-19 Patient Zero is a failure of memory: in my blog, I wrote—because I believed it—that this happened in January. When I subsequently reviewed my records, I came across a photo selfie of me on the nebulizer in a West Hollywood urgent care clinic. It was dated November 15th and I had already been sick for a couple of weeks. You may be less surprised that I made such a mistake when I tell you that my mom was desperately ill at the time, and she died on February 7th after a year of hell. Whatever it was, COVID-19 or something else, definitely happened in November.
Does it matter? Scientifically of course the answer is yes. Epidemiologists benefit when they can trace a viral pandemic to its roots. Personally, medically, probably. Though the experts remain officially uncertain whether someone can be reinfected by COVID-19, the evidence appears to say that COVID-19 survivors probably cannot get reinfected to a significant extent. It wouldn’t prompt me to go out in public without a mask or stop washing my hands. I know it’s selfish but I won’t deny it: I would love the peace of mind of knowing that this particular beast isn’t going to kill me. And I would like to donate blood for use as plasma in order to treat coronavirus victims.
As it stands, most of my thoughts on this subject are a muddled rumination about the nature of humanity and the reliability of personal knowledge. If I were an animal, and had never heard of science, and had memory and self-awareness, I would know—know with the same certainty that I know I am typing this column—that I had COVID-19 and that I should probably worry about something else more than the possibility that I might get it again. But I am not an animal, I am an American filled with self-doubt, in awe of Science and the desire to document what can probably never be proven and that in fact might not be true at all.
(Ted Rall (Twitter: @tedrall), the political cartoonist, columnist and graphic novelist, is the author of the biography “Bernie,” updated and expanded for 2020. You can support Ted’s hard-hitting political cartoons and columns and see his work first by sponsoring his work on Patreon.)

Many Americans bemoan the normalcy before the lockdown prompted by the COVID-19 pandemic. Until we can get back to normalcy, however, we can do all the things that make America America by using technology.
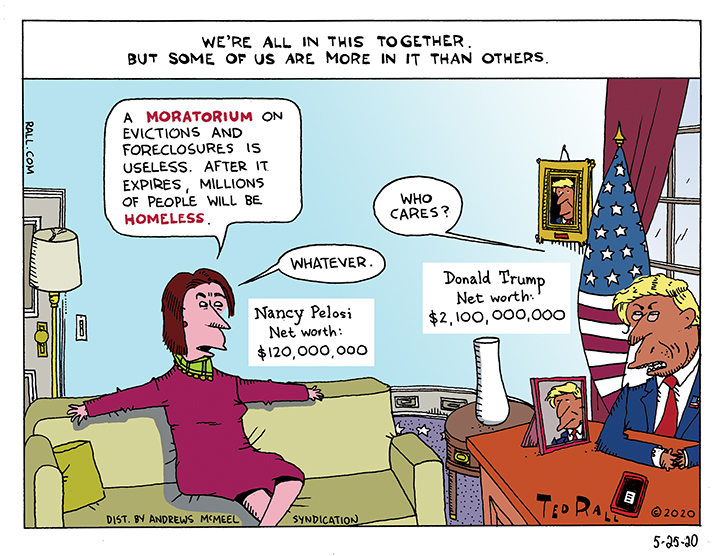
Even liberal Democrats are unwilling to provide real relief to distressed homeowners and renters. All they want to offer is a temporary moratorium on evictions and foreclosures. In that respect, they are exactly the same as the Republicans. After all, they have a common class interest.
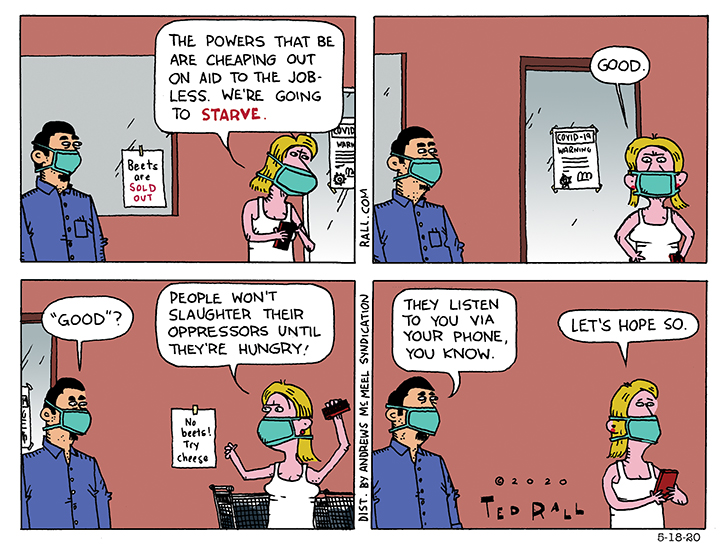
he people, Marxists always said, won’t revolt unless they’re hungry enough. Mass unemployment and poverty, along with government in action, are about to test that proposition.

Feminist who support both the “me too” movement and former vice president Joe Biden’s campaign for president awkwardly respond to rape allegations by Tara Reade.
