Refusing to succumb to panic is laudable and rational, and when the infection rate numbers in the single digits here in the U.S., there’s no reason to freak out. But mainstream media organizations and the government are diminishing their already scant credibility when they downplay the threat of Ebola.
Since a Liberian man appeared at a Dallas hospital and subsequently succumbed to the disease on October 8th, public health officials and reporters have repeatedly stated that Ebola is difficult to catch. Echoing widely circulated information about HIV-AIDS, they’ve told the public that the only way Ebola can be transmitted is through direct contact with bodily fluids.
Technically, this is true.
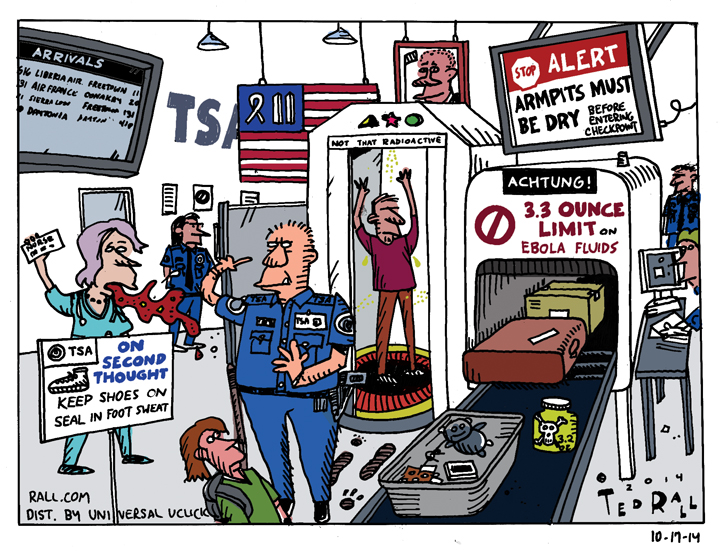
As with the Bush administration’s 2002 buildup to the invasion of Iraq, in which White House officials’ arguments omitted their lack of certainty about Saddam Hussein’s supposed weapons of mass instruction, the official line on Ebola is undermined by a lie of omission. Sweat, you see, is a bodily fluid that can carry Ebola. If you touch a drop of sweat left on, say, the armrest of a seat on an airplane, by a carrier, you have been exposed to Ebola.
CDC and Obama administration officials have been reluctant to talk about this.
A rare exception to the perspiration blackout was an October 27th Congressional hearing, during which expert witnesses confirmed that sweat is included among the infected bodily fluids that transmit Ebola. Rep. Thomas Massey, a Kentucky Republican, asked Department of Health and Human Services assistant secretary Dr. Nicole Lurie if Ebola could survive in perspiration left on an inert surface, like a bus seat, for at least 15 minutes, and then be transmitted to another commuter.
Lurie confirmed that the answer was yes: “it [the Ebola virus] can survive.”
At this point, there is no reason to shut down schools, much less airlines or mass transit. But the political class and the media that serves it are too clever by half if they think Americans don’t notice the omissions and inconsistencies in their official narrative.
Ebola is an extremely dangerous and contagious disease that kills about 50% of those who contract it. America’s post-9/11 airport security apparatus, obsessed with toothpaste and what’s inside your shoes, didn’t have the slightest screening system in place to deal with passengers arriving from West Africa, and even now contents itself with a half-assed temperature check that doesn’t even use reliable thermometers. Obama told us that he had this thing under control, that his team was prepared, but they plainly weren’t – and now that they’re finally paying attention, they’re imposing quarantines that are unnecessary, counterproductive – or voluntary, and thus pointless.
Given how poorly and dishonestly the government has communicated about Ebola, is it any wonder the public doesn’t trust them?
Government officials repeatedly state that Ebola is not an airborne disease. (Obama: “This is not an airborne disease. It is not easy to catch.”) However, the doctors and health workers who became infected while treating Ebola patients in Africa followed CDC protocol, wearing head to toe protective gear. They didn’t notice any tears or gaps. Yet they got the virus anyway. How? They don’t know. Many respected epidemiologists – not crazy right-wing conspiracy theorists – wonder aloud whether airborne transmission has already resulted from an as yet undocumented mutation. It isn’t an outlandish concern. After all, there was a 1989 version of Ebola which spread from monkey to monkey in the air, and a 2012 version – Ebola Zaire, involved in the present outbreak – documented to have spread from pigs to monkeys via the air.
And in a press release studiously ignored by corporate media, the CDC recently clarified a distinction without much of a difference: while it doesn’t consider Ebola an airborne-spread virus, it does consider it a “droplet-spread” virus: “Droplet spread happens when germs traveling inside droplets that are coughed or sneezed from a sick person enter the eyes, nose, or mouth of another person. Droplets travel short distances, less than 3 feet (1 meter) from one person to another. A person might also get infected by touching a surface or object that has germs on it and then touching their mouth or nose.”
On the New York subway, no one gets a three foot radius to themselves.
Why are major television networks and print newspaper outlets continuing to tell us that there’s nothing to worry about, and continuing to imply that it’s as hard to get Ebola as it is to contract HIV-AIDS? If I didn’t know better, I’d say it’s because the government and the media care more about keeping the economy and the Ebola-struck transportation industry humming along than about protecting the American people.
Ironically, there’s no better way to spread panic than to be less than completely truthful.
(Ted Rall, syndicated writer and cartoonist, is the author of the new critically-acclaimed book “After We Kill You, We Will Welcome You Back As Honored Guests: Unembedded in Afghanistan.” Subscribe to Ted Rall at Beacon.)
COPYRIGHT 2014 TED RALL, DISTRIBUTED BY CREATORS.COM